Journal of Abdominal Wall Surgery, 5:16018 (2026)
Intraoperative Fascial Traction - From Concept to Comprehensive Application
Niebuhr, H., Woeste, G., Winkler, C., Behle, S., Reinpold, W., Dag, H., Köckerling, F.
This review paper proposes an algorithmic use of intraoperative fascial traction in complex abdominal wall hernias. Based on defect width and intraoperative findings, traction is applied to assess and optimize medialization before considering additional reconstructive steps. The approach aims to standardize decision-making in CAWR.
Treatment Subgroups by Defect Width:
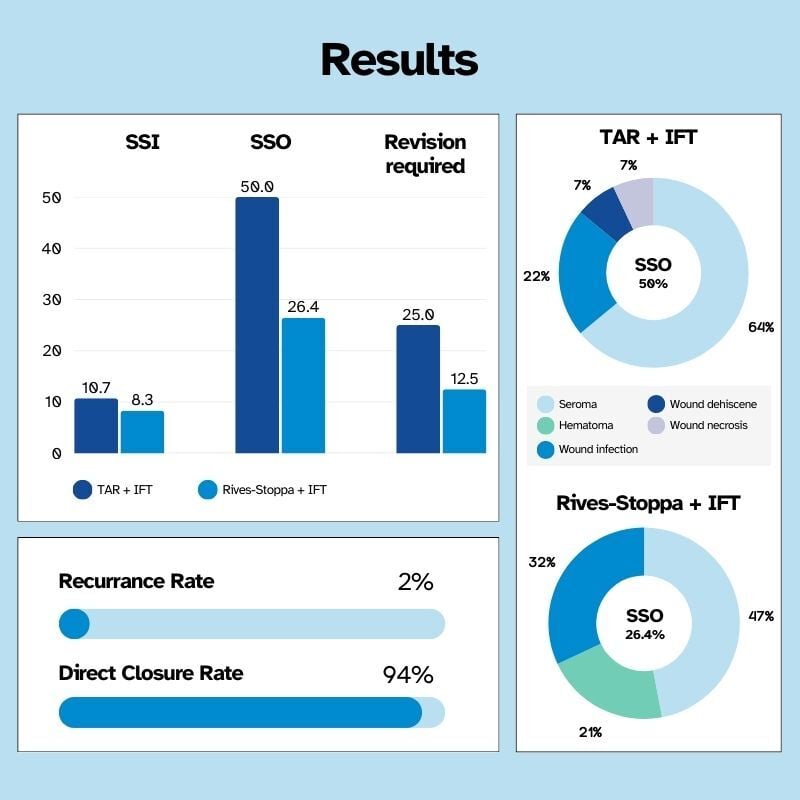
- I: Rives-Stoppa repair forms the surgical base in all defect sizes
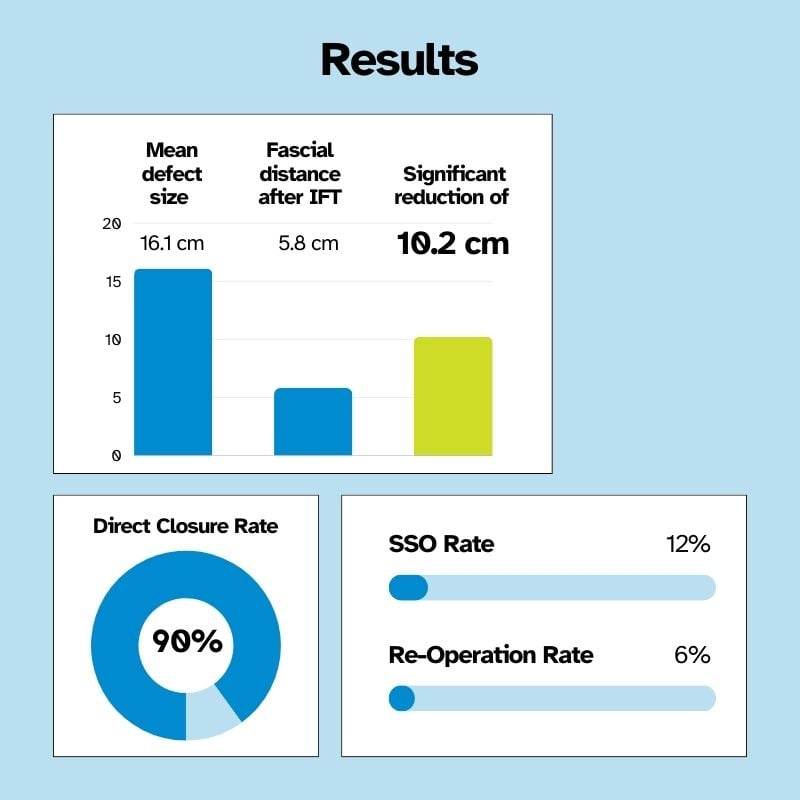
- II: Defect 8 to 19 cm: add IFT to achieve primary fascial closure
- III: Defect > 19 cm: Component separation plus IFT to enable additional medialization






%20-%20Open%20Approach%2015cm_photo8.jpg?width=840&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo8.jpg)