

Clinical Presentation
Initial presentation showing exposed mesh at the umbilicus with surrounding erythema.
Standing Profile
Standing view illustrates the extent of abdominal wall involvement and the hernia bulge.

Pre-operative CT Scan
13.4 cm hernia recurrence with cranial rectus diastasis.
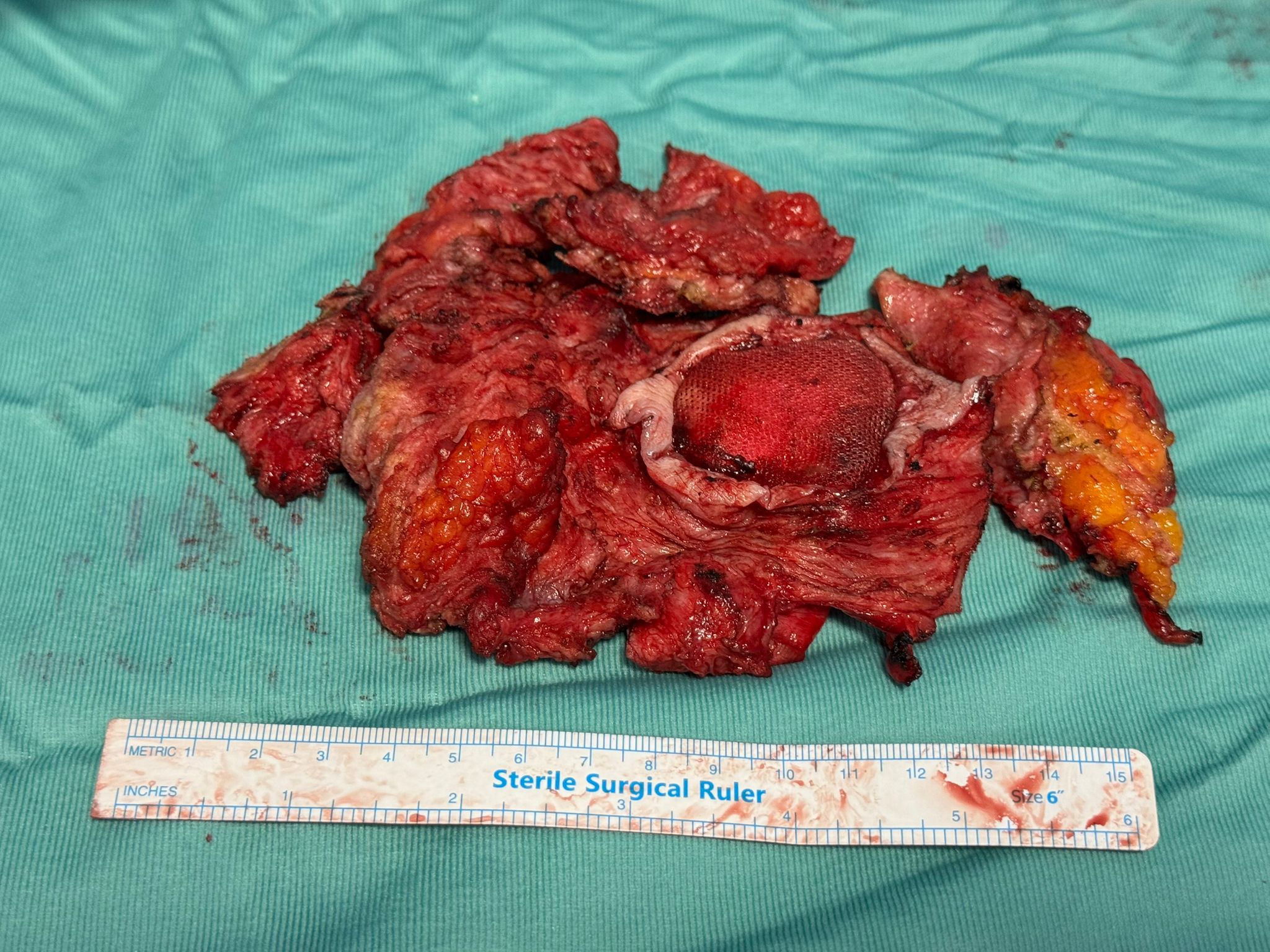
Mesh Explantation
Infected mesh removed en bloc with inflamed overlying skin.
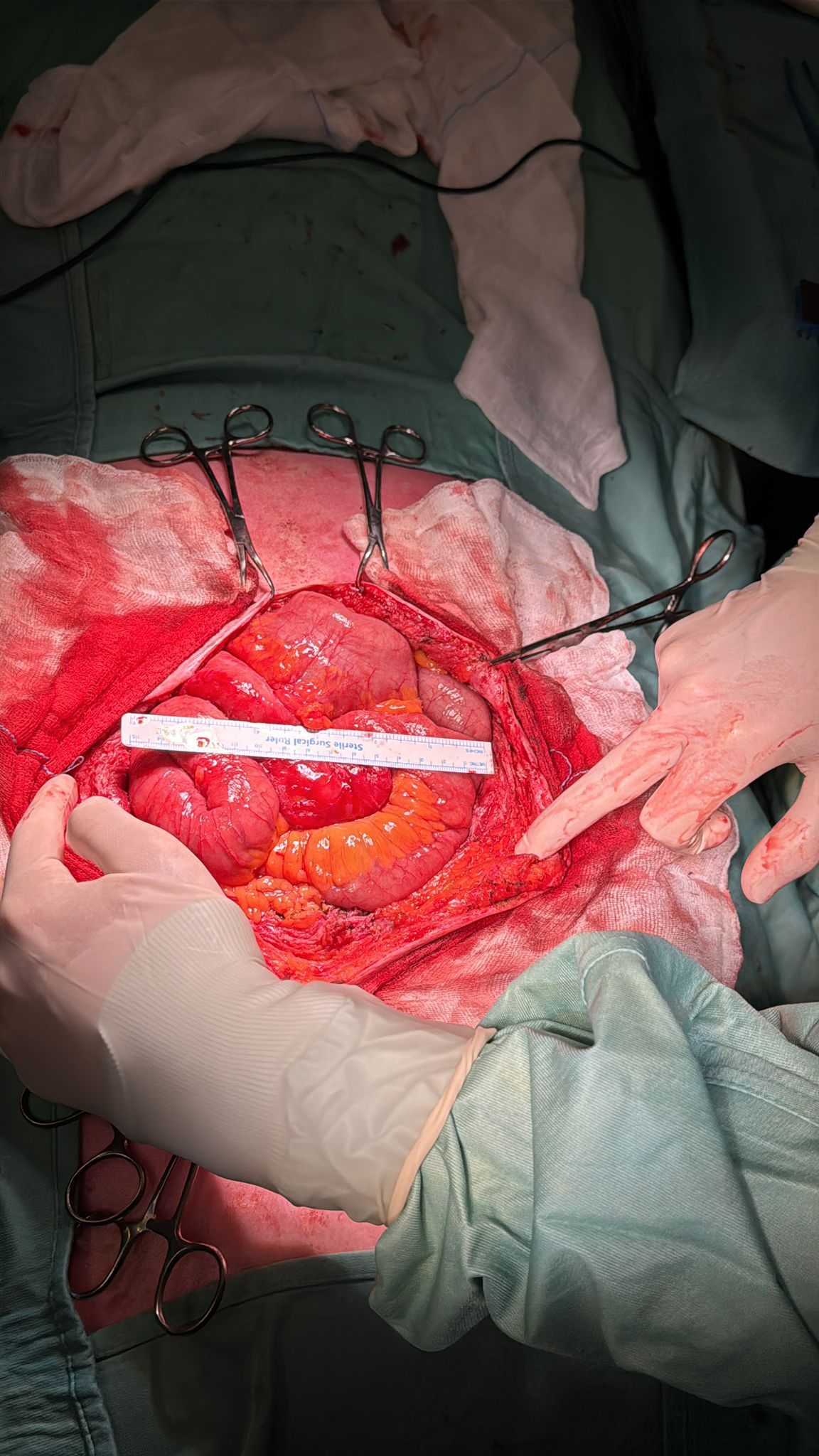
Fascial Defect
15 cm midline gap identified intraoperatively.
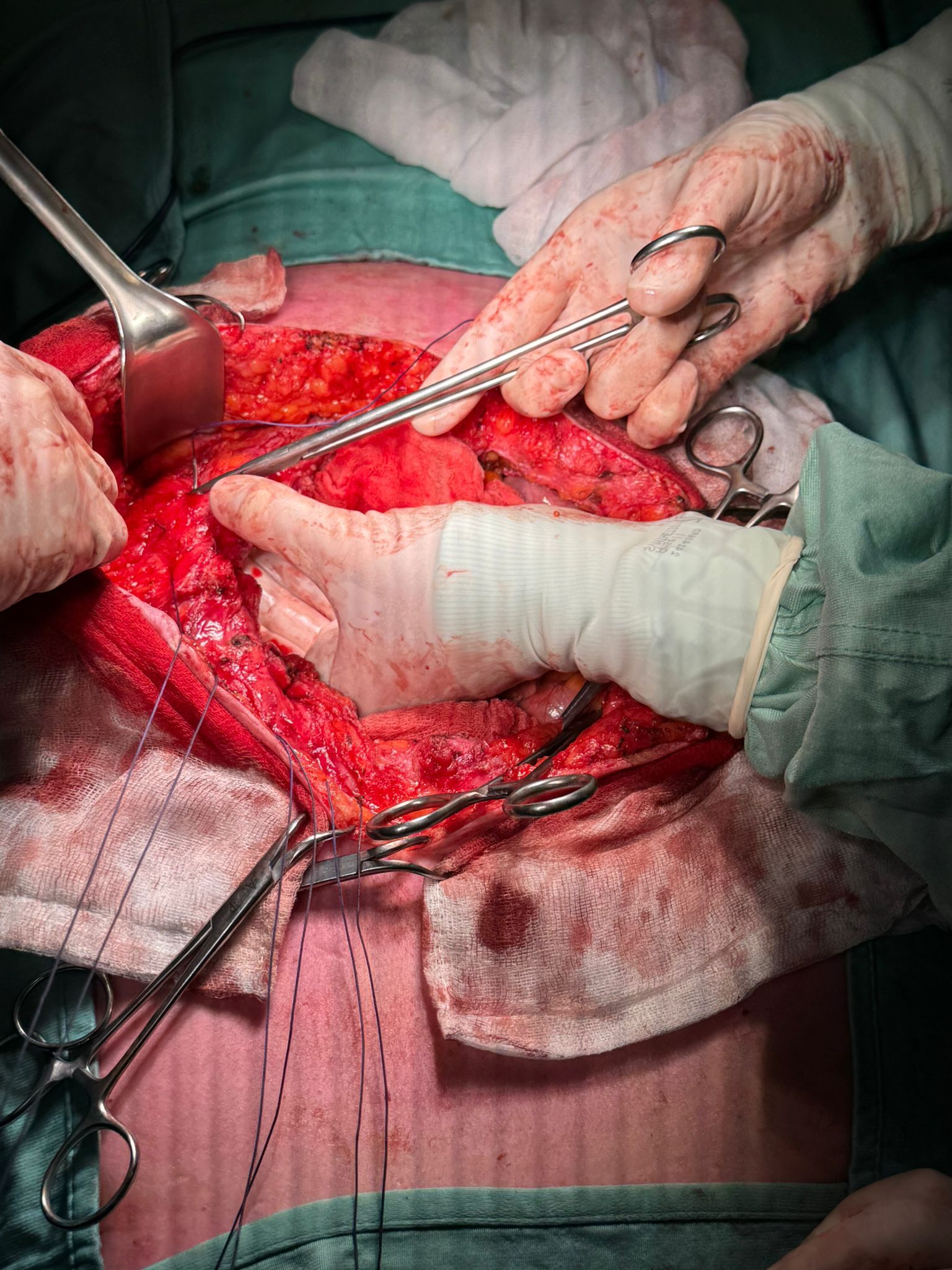
Suture Setup
Sutures placed along fascial edges prior to traction.
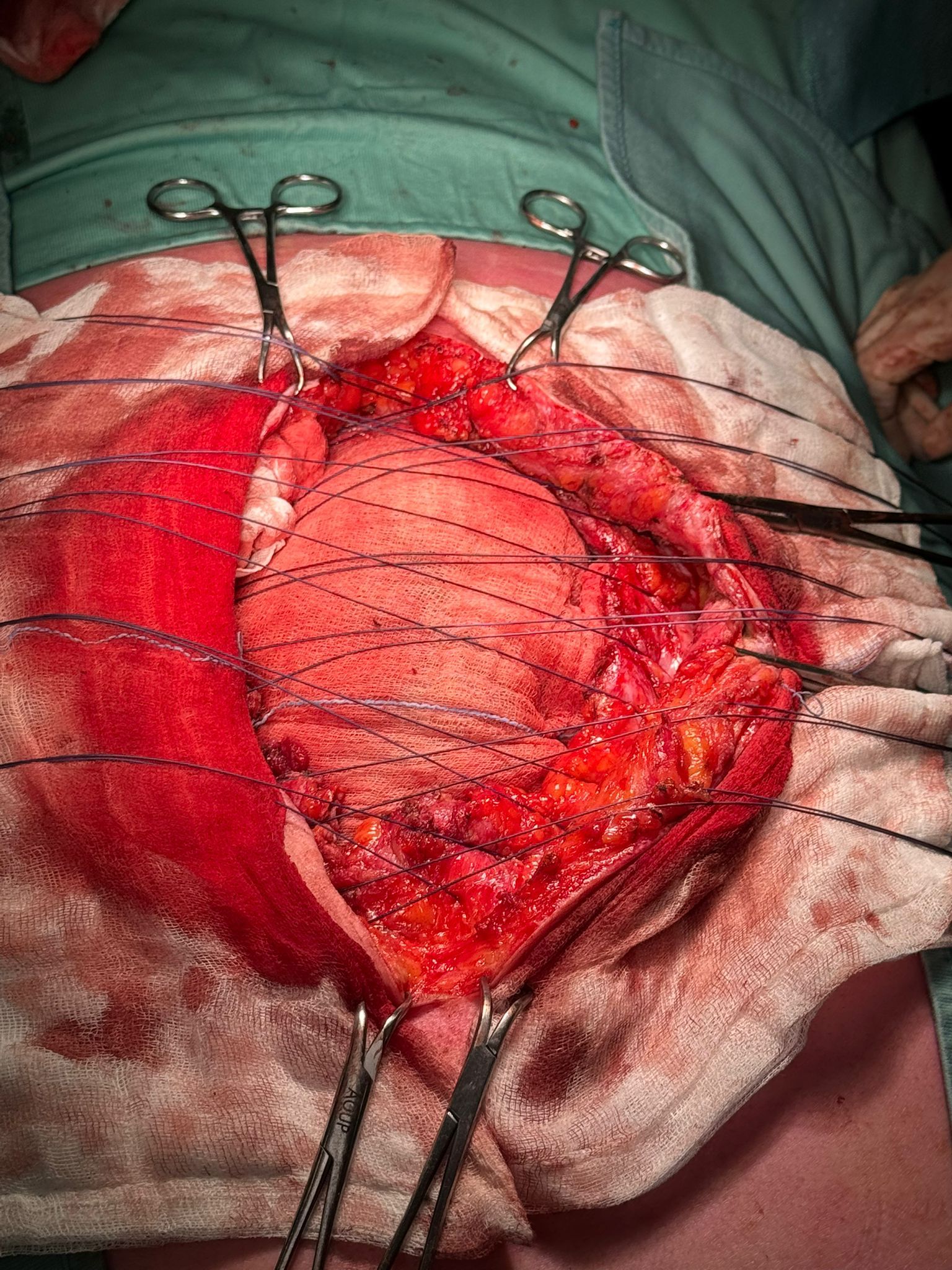
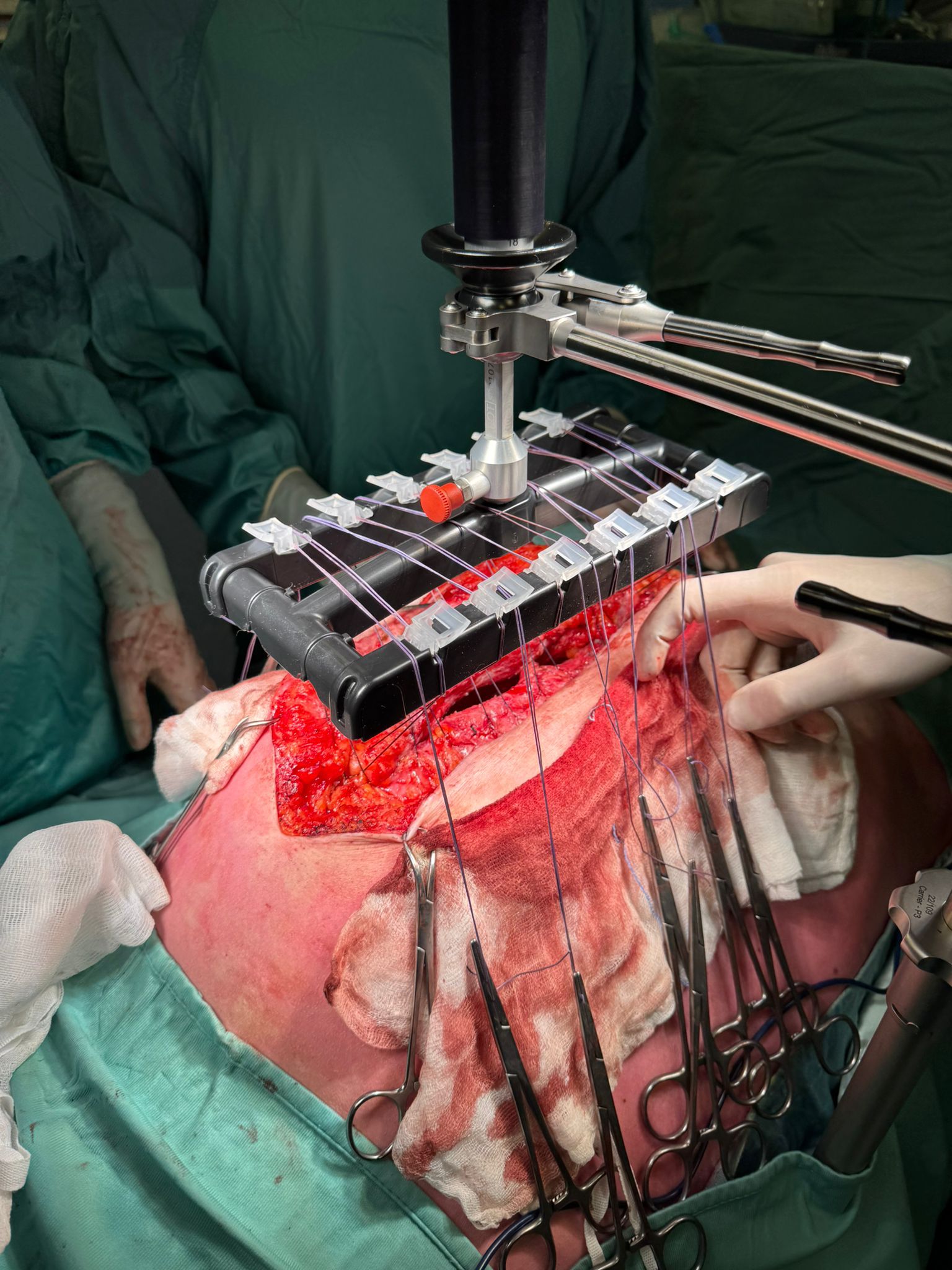
Ready for Traction
Sutures arranged for attachment to fasciotens®Hernia.
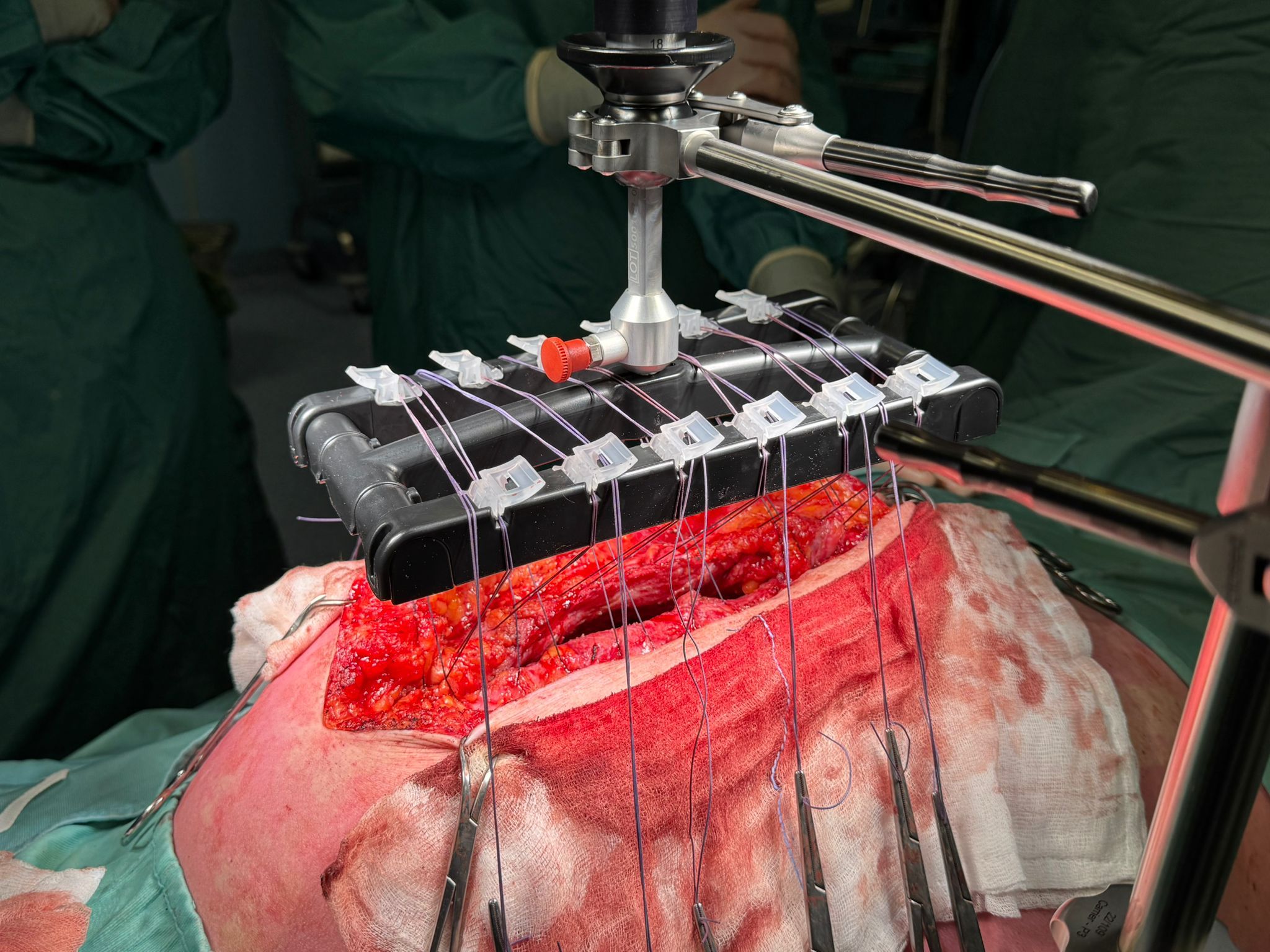
Sutures Secured
Traction applied using fasciotens®Hernia system to elongate abdominal wall
Active Traction
Controlled, dynamic vertical traction applied for 28 minutes.
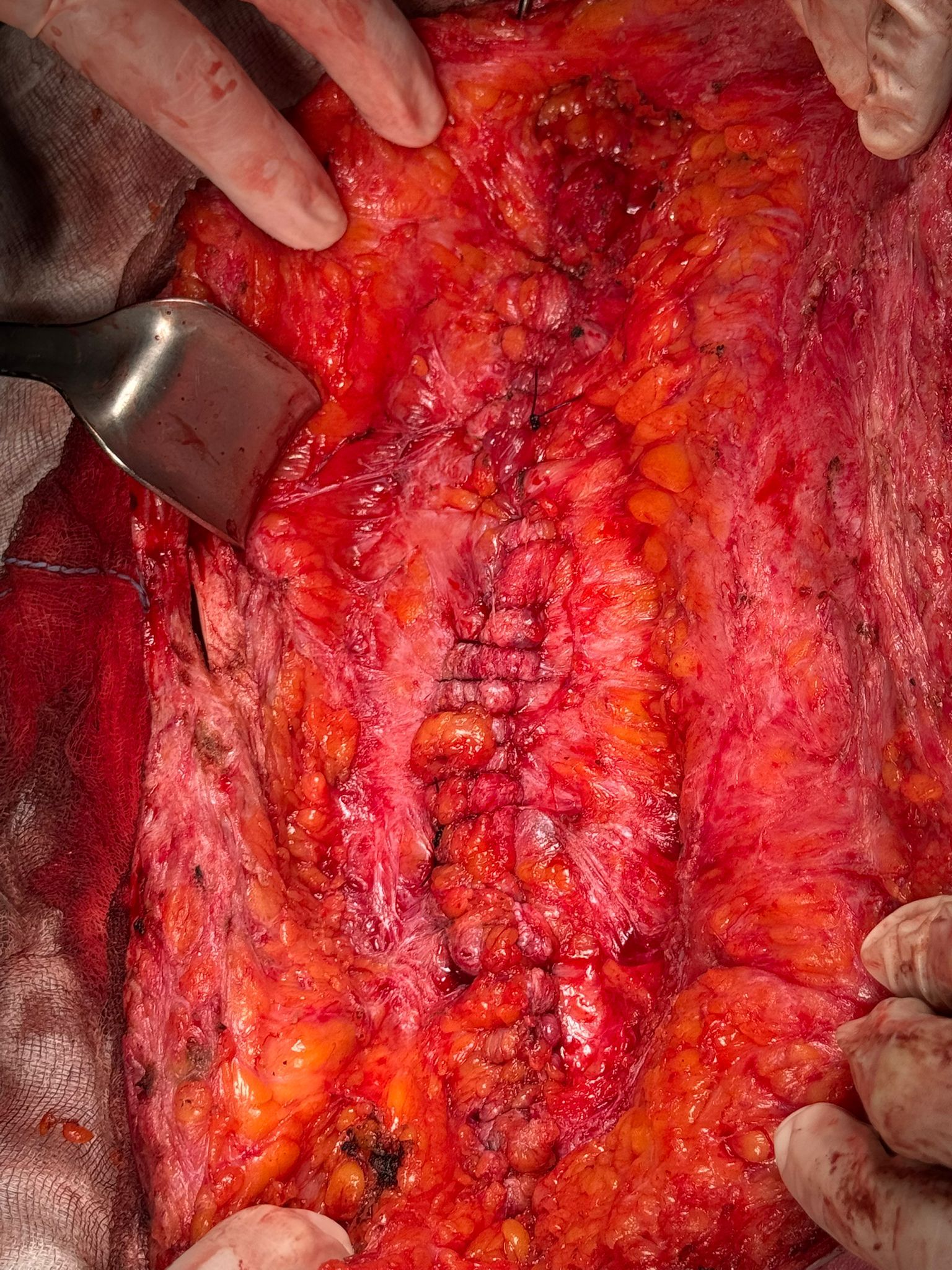
Direct Fascial Closure
Midline successfully re-approximated after IFT.

Final Interoperative View
Completed closure of abdominal wall and skin.