
Preoperative Remarks



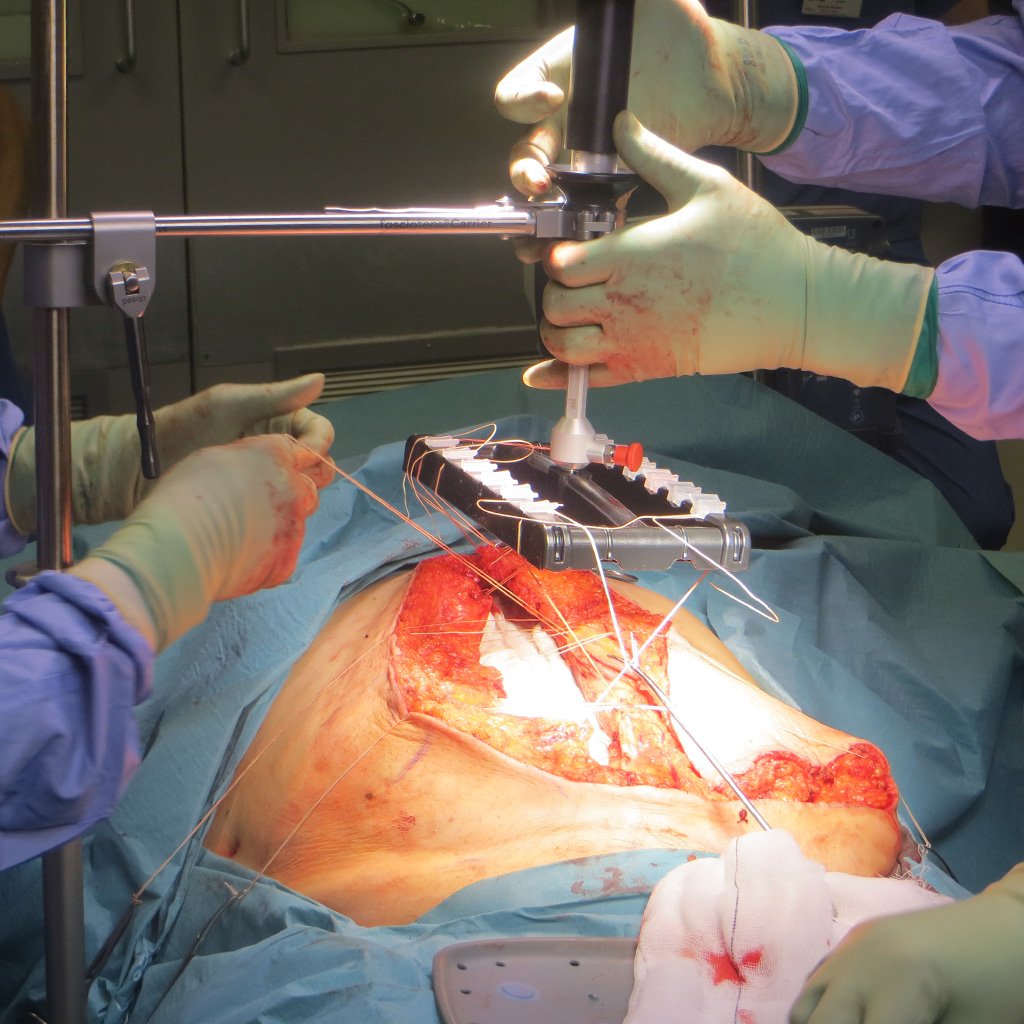
Intraoperative Course

Postoperative Outcomes

The surgeons

Srinivas Chintapatla
Consultant Surgeon – York and Scarborough Teaching Hospital

Tom Macleod
Consultant Plastic, Reconstructive and Cosmetic Surgeon – York and Scarborough Teaching Hospital