%20-%20Open%20Approach%2015cm_photo5.jpg?width=3024&height=4032&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo5.jpg)
---Open-Approach-15cm-Pre-op-CT.gif?width=540&height=476&name=Mahadar-(Mumbai)---Open-Approach-15cm-Pre-op-CT.gif)
Preoperative CT Scan
Cross-sectional imaging prior to repair, demonstrating extensive herniation of abdominal viscera beyond the abdominal cavity, illustrating the degree of loss of domain and the challenge for fascial closure.
---Open-Approach-15cm-Pre-op-coughing_small.gif?width=540&height=540&name=Mahadar-(Mumbai)---Open-Approach-15cm-Pre-op-coughing_small.gif)
Functional Test
Clinical assessment before surgery. With coughing, the hernia sac shows marked outward bulging, highlighting both the size of the defect and the lack of functional abdominal wall support.
%20-%20Open%20Approach%2015cm_photo1.jpg?width=3057&height=3417&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo1.jpg)
Preoperative Planning
Prehabilitative included:
- Botulinum toxin injections for muscle relaxation
-Dietary modification for 5–6 kg weight reduction
-Dobutamine Stress Echo for cardiac clearance.
- hernia boundaries and surgical incision lines were marked on the abdominal wall.
%20-%20Open%20Approach%2015cm_photo4.jpg?width=3024&height=4032&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo4.jpg)
Intraoperative Exposure
Upon entering the abdomen, dense adhesions and the old surgical scar were clearly visualized. Careful dissection was required to avoid injury.
Hernia Sac Mobilization
The hernia sac and surrounding tissue were dissected and mobilized to enable fascial edge visualization and tension-free manipulation.
%20-%20Open%20Approach%2015cm_photo6.jpg?width=3024&height=4032&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo6.jpg)
Fascial Defect Measurement
After adhesiolysis, the fascial gap was measured to be approximately 15 cm wide, confirming the need for additional techniques to achieve fascial closure.
%20-%20Open%20Approach%2015cm_photo7.jpg?width=3024&height=4032&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo7.jpg)
Posterior Rectus Sheath Closure
The posterior rectus sheath was reconstructed using the hernia sac as peritoneal flap to create a retrorectus plane for mesh placement, where a 50x50cm synthetic mesh was placed in a sublay position.
%20-%20Open%20Approach%2015cm_photo8.jpg?width=3024&height=4032&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo8.jpg)
Fascial Traction Evaluation
The (anterior) fascial edges were brought under tension and measured to assess whether midline approximation was possible, still showing a defect and requiring fascial traction.
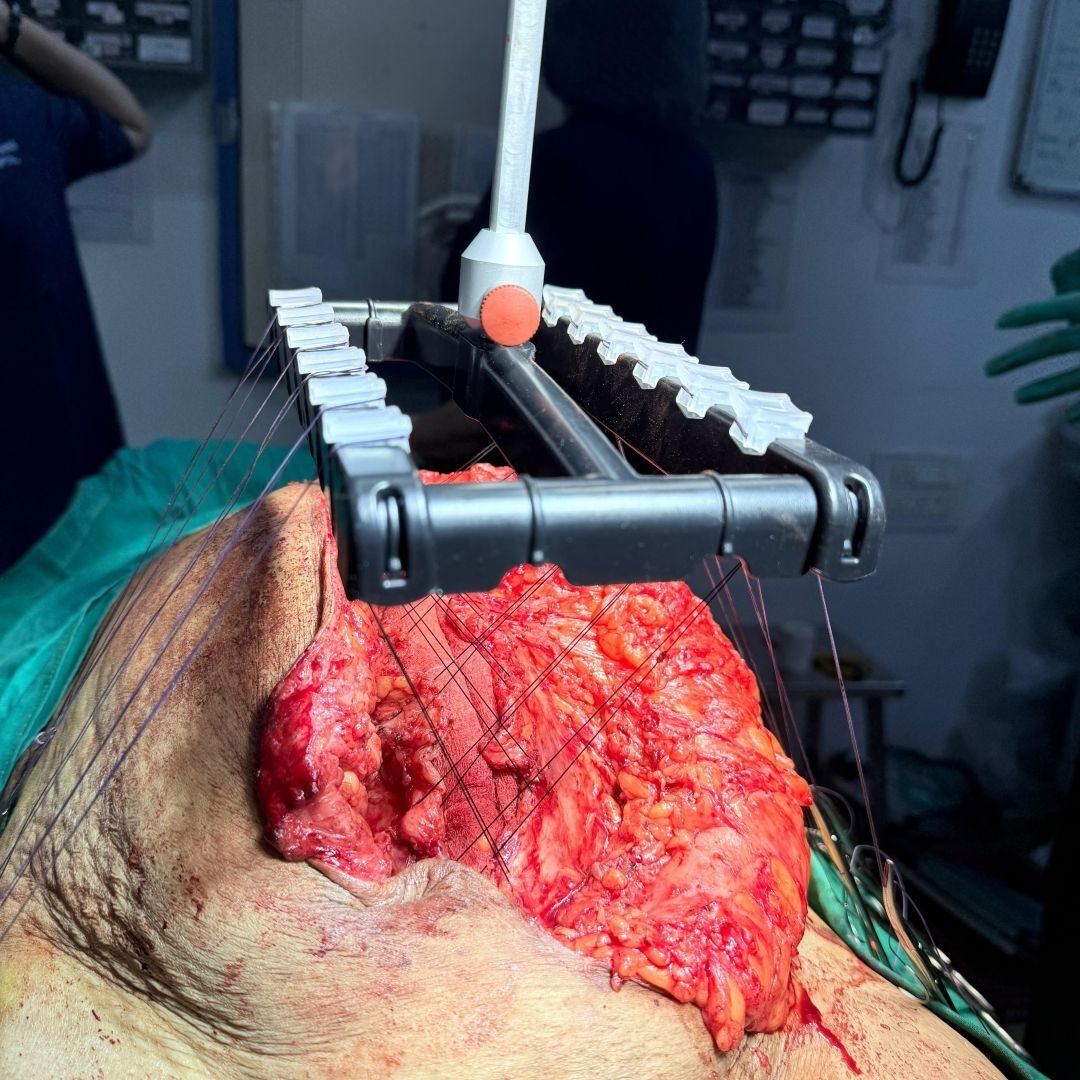
Interoperative Fascial Traction
The fasciotens® hernia device was applied for anterior fascial traction, allowing sucessful low-tension closure of the anterior rectus sheath.
%20-%20Open%20Approach%2015cm_photo10.jpg?width=3120&height=4160&name=Mahadar%20(Mumbai)%20-%20Open%20Approach%2015cm_photo10.jpg)
Skin Closure
The subcutaneous tissue was closed in layers and skin stapled. The patient was extubated on the table and had an uncomplicated recovery. She was mobilized on postop day 1 and discharged home on postop day 7.
---Open-Approach-Post-op-CT.gif?width=540&height=484&name=Mahadar-(Mumbai)---Open-Approach-Post-op-CT.gif)
Postoperative CT Scan
Follow-up imaging after reconstruction. The abdominal contents are restored to their proper position with reestablished midline continuity, showing effective defect closure and restoration of domain.