A 22-year-old patient with a notable medical history of exploratory laparotomy for perforated appendicitis performed four years ago, which was followed by a stormy post-operative course. The patient subsequently developed a hernia at the previous surgical site. Comorbid conditions include poorly controlled diabetes mellitus (initial HbA1c: 11.2 %) and morbid obesity (BMI: 37 at first consultation). Lifestyle factors include chronic smoking and regular alcohol use.

Pre-operative CT Scan
The CT scan shows ventral hernia mainly in the middle and lower part of the abdomen. The hernia sac contains small bowel loops, the rectus muscles and lateral abdominal wall appear intact.
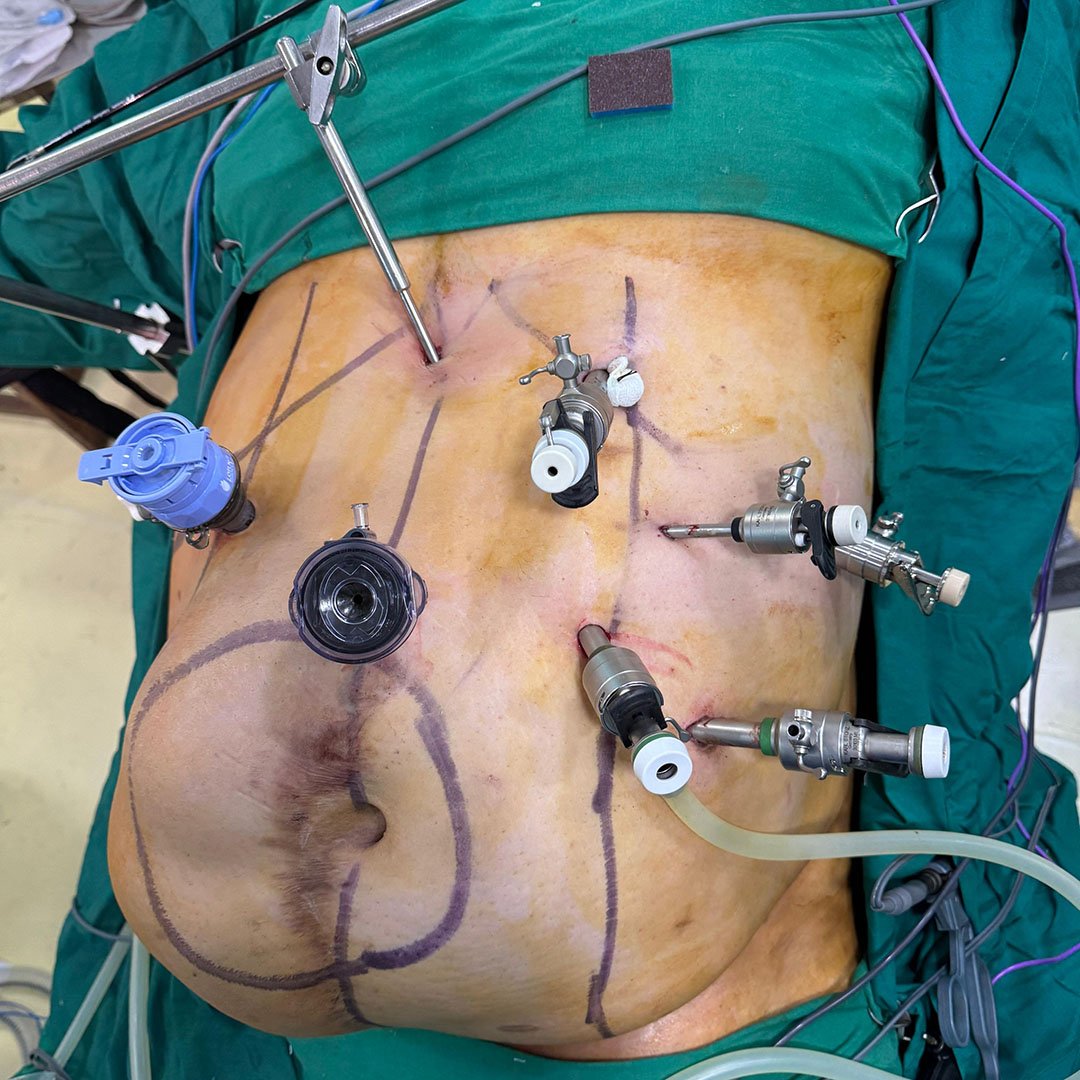
Trocar Placement and Initial Laparoscopic Access
A laparoscopic approach was initiated with multiple ports placed strategically to perform sleeve gastrectomy as well as eTEP dissection. The large right paramedian hernia was mapped on the abdominal wall.
%20Hybrid%20Intraop%204.jpg?width=1600&height=1156&name=Mahadar%20(Mumbai)%20Hybrid%20Intraop%204.jpg)
Laparoscopic Gastric Sleeve
Following trocar placement, a laparoscopic sleeve gastrectomy was performed as the first stage of this combined procedure.
%20Hybrid%20Intraop%201.jpg?width=4032&height=2989&name=Mahadar%20(Mumbai)%20Hybrid%20Intraop%201.jpg)
eTEP
Retrorectus dissection carried out using the eTEP approach, allowing wide exposure of the hernia defect margins and adequate mobilization of the posterior sheath for layered closure.
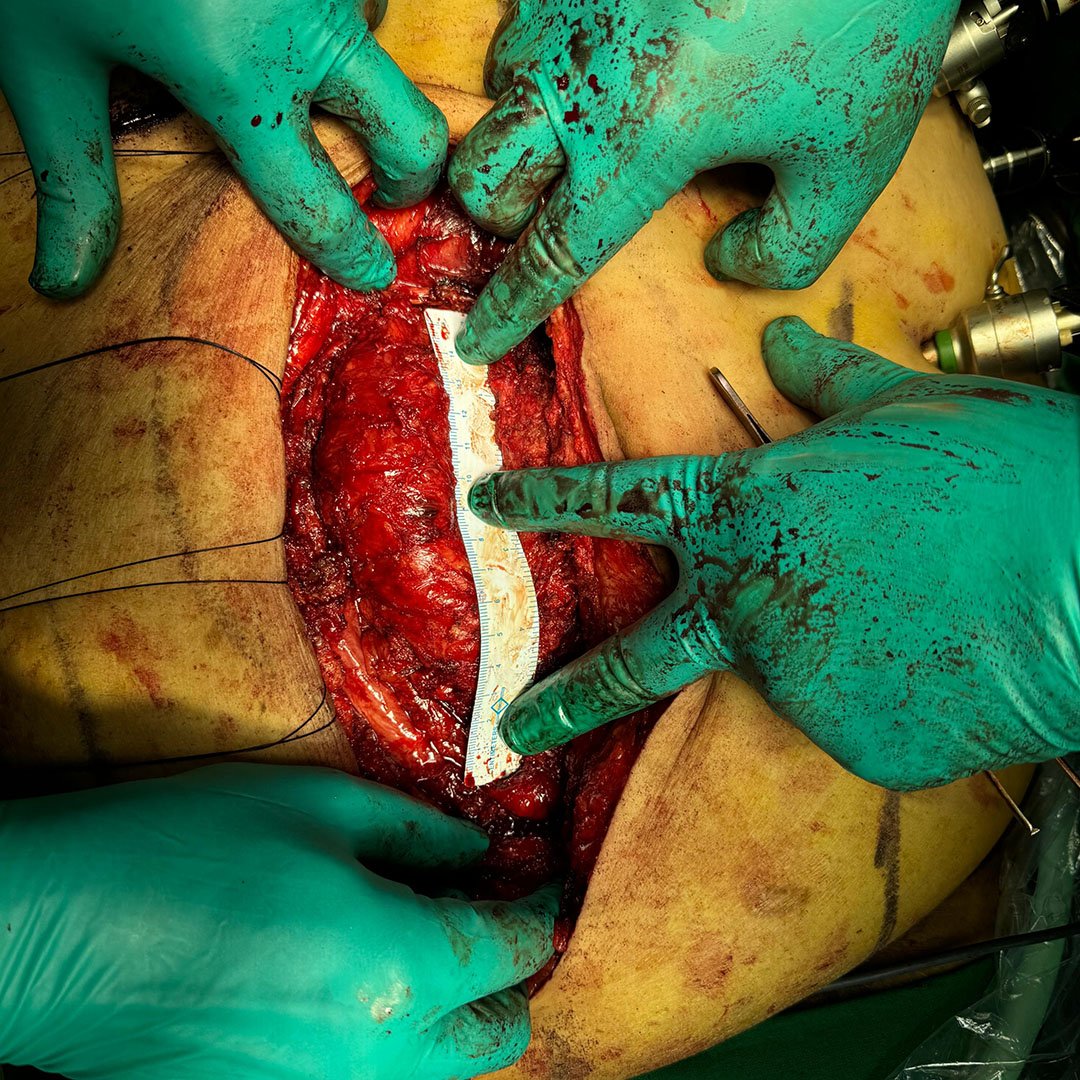
Open Surgery
Open exposure of the hernia sac with posterior dissection and measurement. The hernia sac was initially and the posterior rectus sheath was eventually reconstructed using a peritoneal flap, aided by a right-sided Transversus Abdominis Release (TAR). A mesh was placed in sublay position.
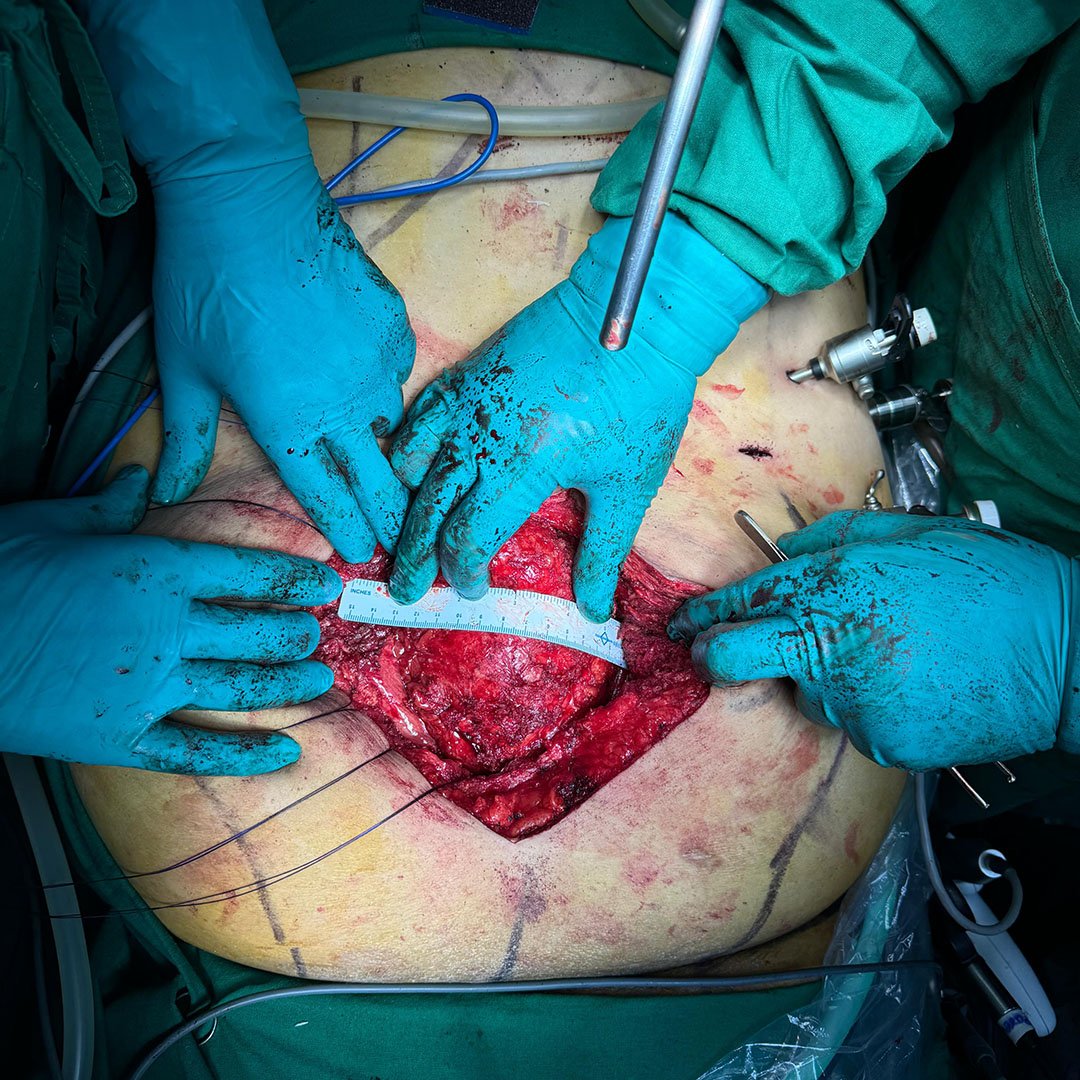
Defect Measurement and Preparation for IFT
At this point, the anterior transverse fascial defect measured approximately 12 cm. The decision was made to apply fasciotens®Hernia to facilitate anterior sheath closure without creating an increase in the intra-abdominal pressure.
IFT Using fasciotens®Hernia
fasciotens®Hernia was mounted and used to apply continuous traction to anterior rectus sheaths. This significantly reduced the fascial gap, enabling complete closure of the anterior layer without bridging.

Fascial Closure and Wound Management
Immediate postoperative view with closure and stapled port sites. The fascia was fully closed, and the anterior sheet approximated without the need of bridging. No increase in ventilation pressures was noted, and the patient remained hemodynamically stable throughout. The patient was extubated on the table and experienced an uneventful recovery. He was mobilized early and discharged on postoperative day 4.
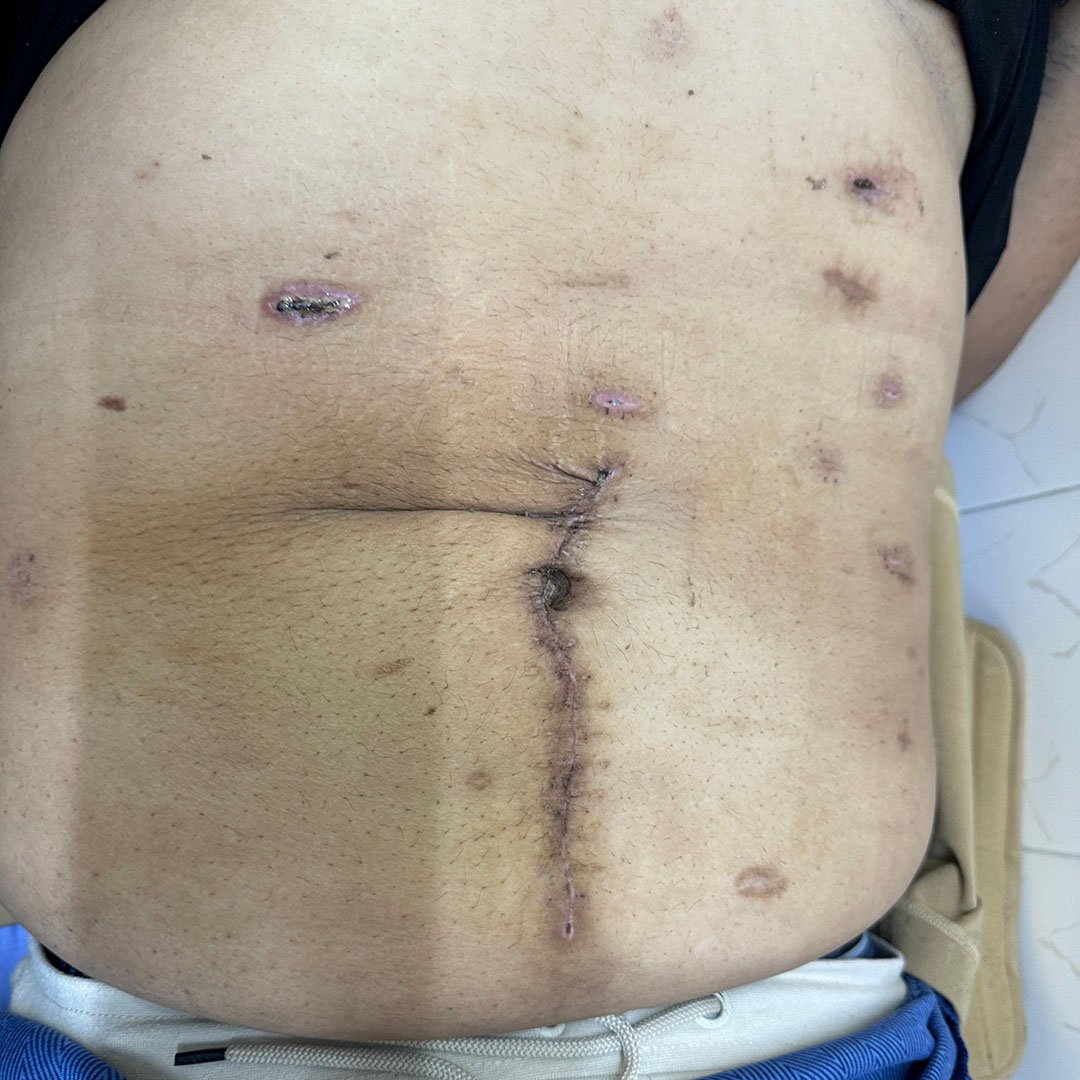
5-months Follow-up
At the 5-months follow-up, his BMI had reduced to 26.4, and his HbA1c was well-controlled at 6.9 %. There was no evidence of a hernia recurrence.