Surgical Steps
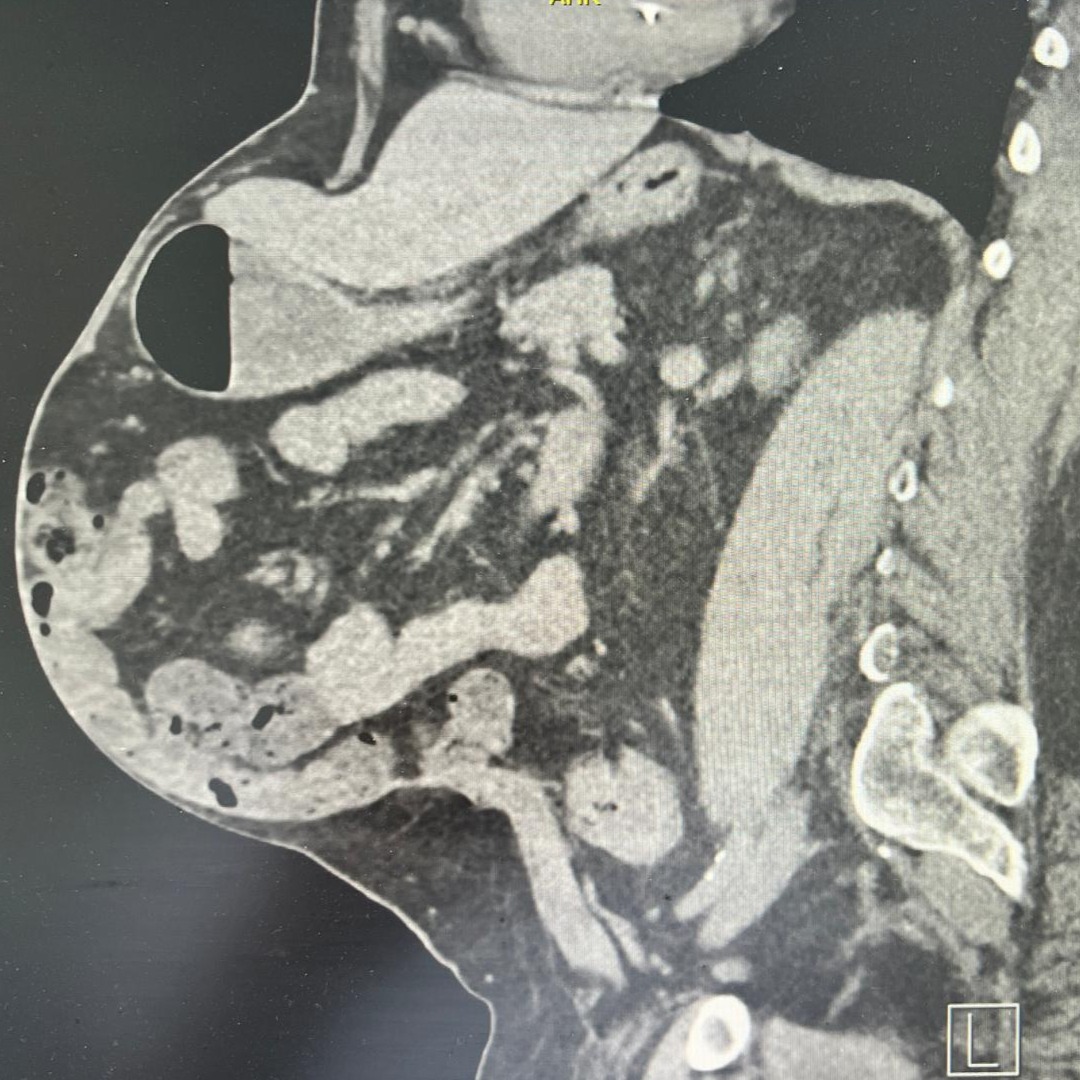
Pre-Operative CT Scan
Large ventral hernia with a defect size of 23 × 23 cm and loss of domain of 28% (EHS-Classification: M2-4W3)

Closure of Posterior Rectus Sheath
Posterior sheath approximation after bilateral transversus abdominis release. Defect size measured 17 cm without tension
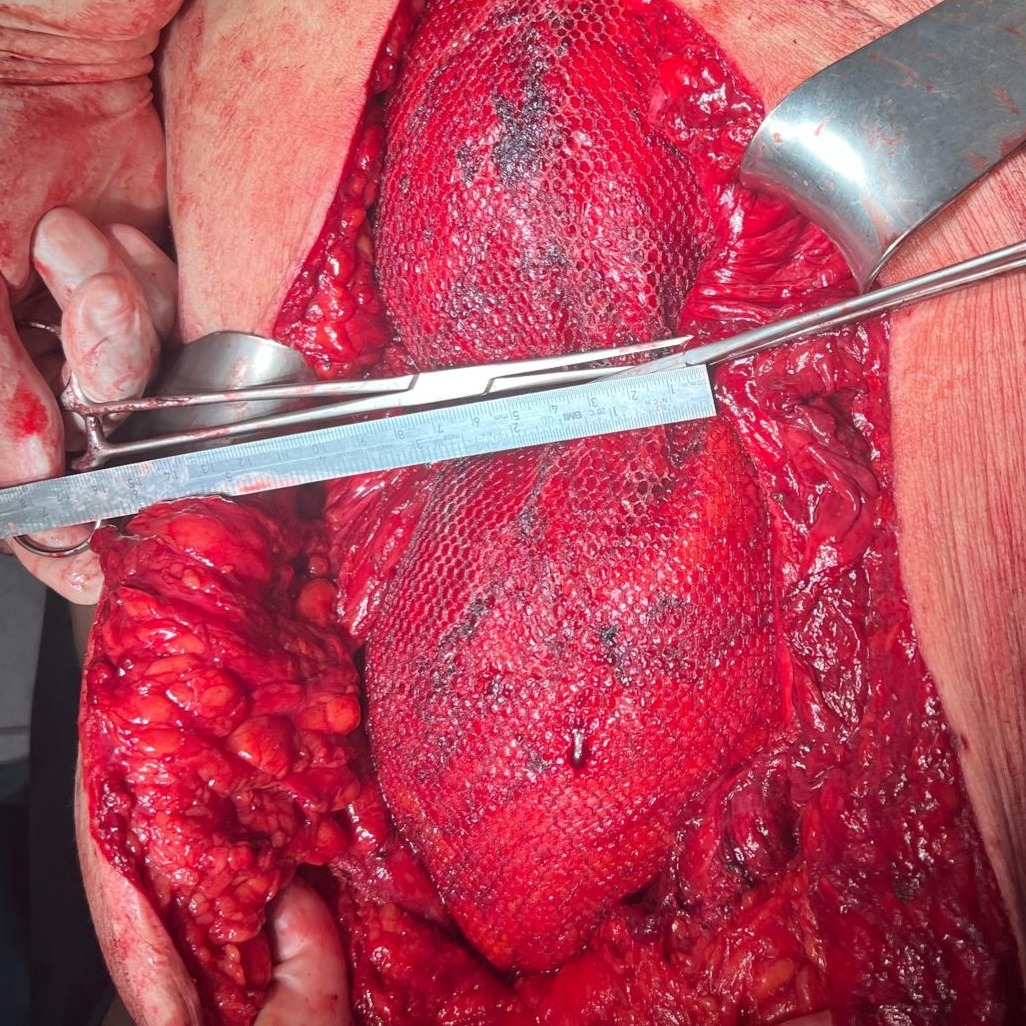
Fascial Defect Measurement
After mesh placement, gap measured at 8–9 cm with manual approximation.
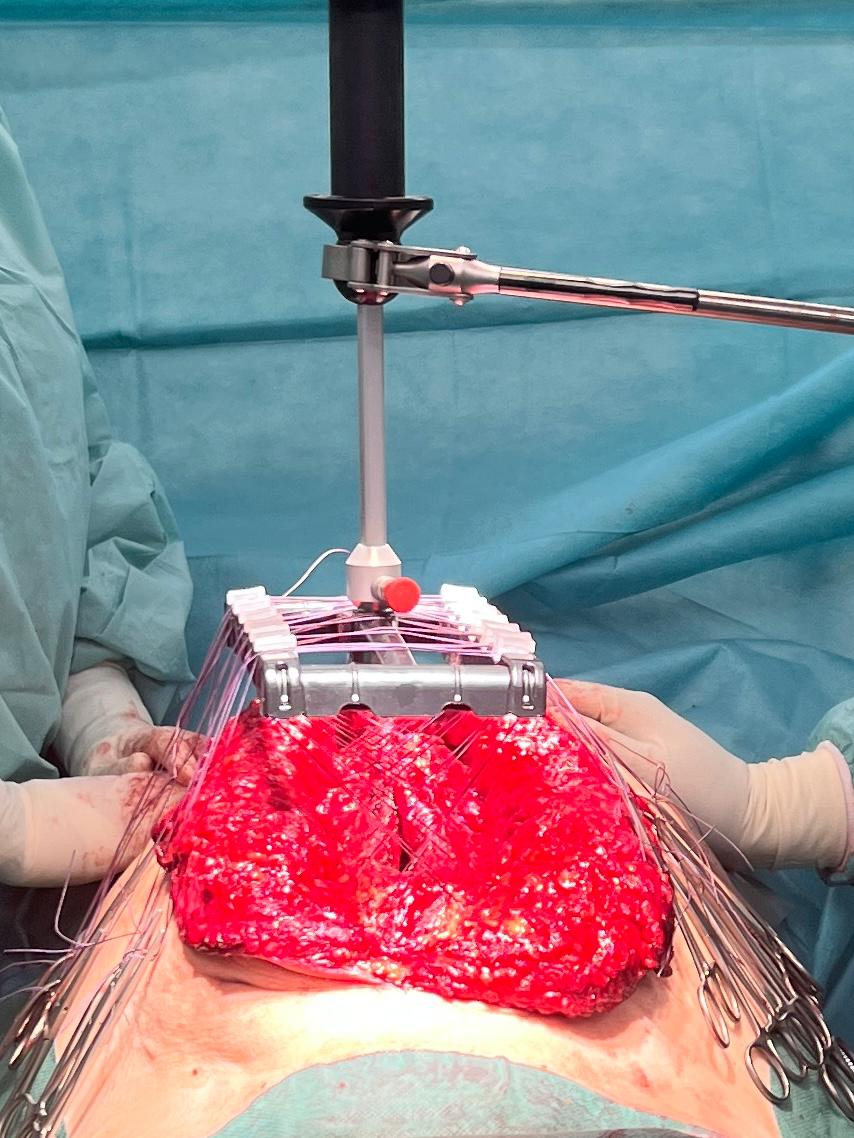
Traction Phase
30 minutes of intraoperative fascial traction applied with forces up to 20 kg.

Completed Anterior Midline Closure
Final midline closure achieved without tension.

Post-Operative Results
Lateral and frontal comparison before surgery and after recovery, showing reduced abdominal protrusion.